Bone marrow is a spongy substance found in the center of the bones. It manufactures bone marrow stem cells and other substances, which in turn produce blood cells. Each type of blood cell made by the bone marrow has an important job.
Red blood cells carry oxygen to tissues in the body.
Platelets stop bleeding by helping blood clot.
White blood cells fight infections.
White Blood Cells
Three very important types of white blood cells are essential to the proper functioning of the body’s immune system, which fights infection:
Neutrophils and Macrophages — These white blood cells fight bacterial and fungal infections by “eating” germs
Lymphocytes — These white blood cells fight bacterial, viral and fungal infections. T lymphocytes, also called T cells, attack viruses and other germs. T cells from the donor also can attack the recipient resulting in a reaction called graft versus host disease. T cells from the recipient can reject the donor bone marrow cell resulting in graft failure. B lymphocytes make antibodies which help destroy germs in our body.
Alternative Sources of Bone Marrow Stem Cells
Another source of bone marrow stem cells is the blood that circulates in the veins and arteries of all normal people. These stem cells are known as peripheral blood stem cells (PBSC). Patients recovering from chemotherapy and healthy people who are treated with certain drugs that stimulate the growth of the bone marrow have relatively large numbers of PBSC in their blood. The PBSC can be collected and used in certain situations as a source of stem cells for transplantation.
Another source of stem cells is the blood found in the placenta of a newborn baby once the umbilical cord is cut. Umbilical cord blood (UCB) has been successfully used as a source of bone marrow stem cells for transplantation in both related and unrelated patients.
UCSF Benioff Children’s Hospitals medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your child’s doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your child’s provider.
Disclaimer: This article has been taken from https://www.ucsfbenioffchildrens.org/ as it is. Click here to read the original article.
Lung cancer occurs when cells divide in the lungs uncontrollably. This causes tumors to grow. These can reduce a person’s ability to breathe and spread to other parts of the body.
Lung cancer is the third most commonTrusted Source cancer and the main cause of cancer-related death in the United States. It is most common in males, and in the U.S., Black males are around 15% more likely to develop it than white males.
Smoking is a major risk factor, though not everyone who develops lung cancer has a history of smoking.
Lung cancer can be fatal, but effective diagnoses and treatments are improving the outlook.
This article will explain what lung cancer is, how to recognize the symptoms, and the treatment options available.
What is lung cancer?
Cancer causes changes in cells that are otherwise healthy. The cells grow too quickly, without dying off.
Normal cells in the body usually die at a certain stage in their life cycle, thereby preventing a buildup of too many cells. In cancer, however, the cells continue to grow and multiply. As a result, tumors develop.
The two main types of lung cancer are small cell lung cancer and non-small cell lung cancer, depending on how they appear under a microscope. Non-small cell lung cancer is more common than small cell lung cancer.
Anyone can develop lung cancer, but cigarette smoking and having exposure to smoke, inhaled chemicals, or other toxins can increase the risk.
To discover more evidence-based information and resources for healthy aging, visit our dedicated hub.
Types
The main types of lung cancer are non-small cell lung cancer and small cell lung cancer. They differ in the size of cell, as seen under a microscope.
Non-small cell lung cancer
Around 84% of lung cancer cases in the U.S. are non-small cell. There are three subtypes:
adenocarcinoma
squamous cell cancer
large cell carcinoma
Small cell lung cancer
Around 13% of lung cancer cases in the U.S. are small cell. This type tends to grow more quickly than non-small cell lung cancer.
Symptoms and signs
People with lung cancer may not have any symptoms until a later stage. If symptoms do appear, they can resemble those of a respiratory infection.
The staging of cancer describes how far it has spread through the body and how severe it is. Staging helps healthcare professionals and individuals decide on a suitable course of treatment.
The most basic form of staging is as follows:
localized, wherein the cancer is within a limited area
regional, wherein the cancer has spread to nearby tissues or lymph nodes
distant, wherein the cancer has spread to other parts of the body
Similar to this is the TNM staging system. Healthcare professionals assess the tumor for size and spread, whether or not it affects the lymph nodes, and whether or not it has spread elsewhere.
There are also specific ways of staging non-small cell and small cell lung cancer.
Healthcare professionals typically use tumor size and spread to describe the stages of non-small cell lung cancer, as follows:
Occult, or hidden: The cancer does not show up on imaging scans, but cancerous cells might appear in the phlegm or mucus.
Stage 0: There are abnormal cells only in the top layers of cells lining the airways.
Stage 1: A tumor is present in the lung, but it is 4 centimeters (cm) or under and has not spread to other parts of the body.
Stage 2: The tumor is 7 cm or under and might have spread to nearby tissues and lymph nodes.
Stage 3: The cancer has spread to lymph nodes and reached other parts of the lung and surrounding area.
Stage 4: The cancer has spread to distant body parts, such as the bones or brain.
Stages of small cell lung cancer
Small cell lung cancer has its own categories. The stages are known as limited and extensive, and they refer to whether the cancer has spread within or outside the lungs.
In the limited stage, the cancer affects only one side of the chest, though it might already be present in some surrounding lymph nodes.
Around one-third of people with this type find out that they have cancer when it is in the limited stage. Healthcare professionals can treat it with radiation therapy as a single area.
In the extensive stage, the cancer has spread beyond the one side of the chest. It may affect the other lung or other parts of the body.
Around two-thirds of people with small cell lung cancer find out that they have it when it is already in the extensive stage.
Survival rates
According to the American Cancer Society, the chances of surviving for 5 years or longer after receiving a diagnosis of lung cancer are as follows.
The percentages reflect the chances of a person surviving with lung cancer compared with the chances of a person surviving without lung cancer.
Non-small cell lung cancer
Localized
63%
Regional
35%
Distant
7%
Overall
25%
Small cell lung cancer
Localized
27%
Regional
16%
Distant
3%
Overall
7%
Screening
Undergoing regular screening may be a good idea for people with a high risk of developing lung cancer. Screening is with a low-dose CT scan.
has a history of heavy smoking (30 pack years, which is one pack per day for 30 years or two packs per day for 15 years)
currently smokes or has quit smoking within the past 15 years
Insurance will often cover this screening if a person is aged 55–80 years and has private health insurance or is aged 55–77 years, has Medicare, and meets all the other criteria.
However, people should check with their insurance company before signing up for lung cancer screening.
Diagnosis
If a person has any symptoms that could indicate lung cancer or if screening shows something unusual, a healthcare professional will likely recommend some diagnostic tests.
Imaging tests
An X-ray, CT, MRI, or PET scan might reveal areas of lung tissue with cancer.
If the cancer has spread, imaging tests can also reveal changes to bones and other organs. Scans can also help track the progress of treatment.
Tissue sampling
A healthcare professional may wish to take a biopsy to check for cancer cells. They will do this using a fine needle or a bronchoscope.
A bronchoscope is a thin, lighted scope with a camera on the end that enters the lungs through the mouth or nose. A healthcare professional can use it to look for lesions and take samples.
For less accessible lesions, they may use a more invasive surgical procedure, such as thoracoscopy or video-assisted thoracic surgery, to remove lung tissue.
Other samples
Laboratory tests can also reveal whether or not cancer is present in the:
pleural effusion, which is the fluid that collects around the lungs
sputum
blood
This information can help confirm if cancer is present and, if it is, determine its type and stage.
Treatment
Treatment will depend on various factors, including:
the type of cancer
the location and stage
the person’s overall health
their individual preferences
All the treatment options can have adverse effects. A person should speak with their healthcare professional about the most suitable choice for them, including the pros and cons of each option.
Some treatment options include:
surgery to remove part or all of a lung
chemotherapy, which refers to a drug treatment that can kill cancer cells and shrink tumors
radiation therapy, which uses high energy rays to kill cancerous cells
radiofrequency ablation, wherein a healthcare professional inserts a thin needle and uses an electric current to destroy cancer cells
targeted therapy, which targets a specific behavior to prevent tumor growth
immunotherapy, which helps the body fight cancer cells
palliative therapy, including pain relief, oxygen therapy, and other help that a person may need to manage their symptoms
A healthcare professional will work with the individual and adjust their treatment plan as their needs change.
Outlook
Lung cancer can be fatal, but emerging treatments mean that many people now survive and recover from lung cancer, especially if they receive an early diagnosis.
Some factors affecting the likelihood of a positive outcome include:
a person’s overall health
their age
the stage of cancer at diagnosis
the type of cancer they have
It is not possible to predict exactly how cancer will affect an individual, but a healthcare professional can help a person understand what they may be able to expect by looking at the results of tests and other factors.
Summary
Lung cancer is a potentially fatal type of cancer, but people who receive an early diagnosis often have a good chance of survival.
People with a high risk of developing lung cancer may wish to consider undergoing regular screening. This can detect the early signs and allow for treatment before the cancer spreads.
Anyone who has concerns about their risk of lung cancer should talk with their healthcare professional.
Disclaimer: This article has been taken from https://www.medicalnewstoday.com/ as it is. Click here to read the original article.
There are several different types of surgery offered to treat knee arthritis. Which surgery, if any, is recommended will depend on several factors, such as the patient’s age, anatomy, general health, lifestyle, and personal preferences, as well as the surgeon’s experience and preferences.
Total Knee Replacement Surgery (Total Knee Arthroplasty)
Patients with moderate to severe knee arthritis who have exhausted non-surgical treatment options might consider replacing the entire knee joint. The surgery involves cutting the arthritically damaged ends of the tibia (shin bone) and femur (thighbone) and capping both with prostheses (like capping teeth).
The two prosthetic pieces are made of either metal or a durable plastic called polyethylene. These new surfaces move smoothly against one another, creating a functional knee joint. Partial recovery typically takes 4 to 6 weeks1 and full recovery may take a few months to an entire year.
Total knee replacement surgery provides most patients with pain relief and improved knee joint function. However, a replacement knee is not as strong and durable as a healthy knee, and patients are strongly advised not to engage in high-impact activities (such as jogging) that may speed up the wear-and-tear of the new joint.
Partial Knee Replacement Surgery (Unicompartmental Knee Arthroplasty)
Partial knee replacement, often called unicompartmental knee replacement, involves replacing only one of the knee’s three “compartments”:
The medial compartment refers to the inner knee (where a person’s knees touch when the legs are together).
The lateral compartment refers to the outer knee.
The patellofemoral compartment is at the front of the knee, where the patella (kneecap) meets the femur (thighbone).
Partial knee replacement surgery treats the arthritically damaged compartment of the knee joint (typically the lateral or medial compartment) while preserving healthy areas. This surgery is appropriate for only a small number of people, and patients may be ineligible if their knees are not well aligned (e.g. bowlegged or knock-kneed), have severe knee stiffness, have ligament damage, or if they suffer from inflammatory arthritis, such as rheumatoid arthritis.
Compared to total knee replacement, partial knee replacement is less invasive, so it is usually less painful and requires less recovery time. However, partial knee replacement is not as reliable as total knee replacement for alleviating pain.
During a knee osteotomy, a small wedge of natural bone graft or artificial bone material is inserted in the bone to realign the joint. ReadKnee Osteotomy Surgery
This surgery is appropriate for a limited number of younger (under age 60 or so), physically active people whose poor knee alignment has caused a great deal of wear-and-tear on just one side of the knee joint, a condition called unilateral knee arthritis or asymmetrical knee arthritis.
During knee osteotomy the surgeon cuts into the femur (thigh bone) or tibia (shin bone) and either:
Removes a small wedge of bone, or
Adds a small wedge of natural bone graft or artificial bone material.
Knee osteotomy re-aligns the joint to shift more pressure onto the “good” side of the knee joint and reduce wear and tear on the bad side. The goal is to reduce pain and perhaps slow down the progression of knee osteoarthritis. A successful knee osteotomy surgery can postpone the need for total knee replacement surgery up to 10 years.2
Unlike after total knee replacement, recovered knee osteotomy patients may participate in high-impact sports.3 This is a major surgery with potential risks and complications, and patients must be committed to extensive post-surgical physical therapy. A full recovery may take months or even an entire year.4
In arthroscopic surgery, the surgeon inserts a video camera and surgical tools through small incisions and can make an assessment of arthritic joint degeneration.
Arthroscopic surgery requires only small incisions through which the surgeon inserts a very small video camera and surgical tools. During knee arthroscopy, a surgeon can make an assessment of joint degeneration due to arthritis.
The surgeon can also perform knee debridement and lavage, which includes the following process:
Remove loose pieces of cartilage or bone (loose osteophytes) suspected of causing irritation
Trim or smooth out cartilage that has grown irregular and bumpy
Remove inflamed synovial tissue
Flush the joint with a saline solution, a process called lavage, to clean out materials known to cause irritation and swelling
Experts’ opinions differ on whether knee arthroscopy is a worthwhile treatment option for knee osteoarthritis. Some experts point to clinical studies that suggest knee arthroscopy does not provide benefit to knee osteoarthritis patients.5,6 Others reason that because knee arthroscopy is less invasive and carries fewer risks it is worth trying before embarking on a more invasive surgery, such as total knee arthroplasty.7 (Most experts do agree arthroscopy is useful for treating other knee problems, such as repairing meniscal tears.) Knee arthroscopy is an outpatient procedure, but it is still surgery and it can take 6 to 8 weeks for the joint to fully recover.
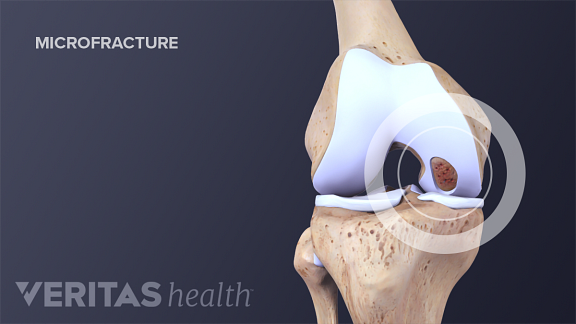
Cartilage Repair and Cartilage Restoration
One way to stimulate cartilage growth is by making precise microfractures in the surrounding bone.
This procedure is called bone marrow stimulation.
Once damaged, cartilage does not heal well. Even if the joint is able to grow new cartilage, it tends to be rough and bumpy and therefore less able to facilitate smooth movement at the joint. There are a handful of surgeries that attempt to repair or encourage the growth of healthy cartilage:
Bone marrow stimulation, which stimulates cartilage growth by making precise microfractures in the surrounding bone
Osteochondral transplantation techniques (OATS), also referred to as “mosaicplasty,” which involves transplanting cartilage from one site to another
Autologous chondrocyte implantation (ACI), which requires two surgeries. In the first, cartilage cells are harvested and then grown in a laboratory for several weeks. During the second surgery the cartilage cells are re-implanted.
These procedures may be appropriate for patients who have a relatively small and very isolated area of articular cartilage damage. Typically, these patients are younger and have damaged their cartilage through trauma (e.g. a sports injury) rather than over years of gradual wear and tear. Therefore, these surgeries are usually more appropriate for people trying to slow or prevent severe arthritis rather than alleviate it.
This article focuses on the most common types of knee surgery for arthritis. New types of surgery, less invasive surgical techniques, and new implant designs and materials are the subjects of ongoing research.
People suffering from knee arthritis should make a concerted effort to alleviate symptoms with non-surgical treatments. If non-surgical treatments do not provide satisfactory pain relief and improved knee function, then an orthopedic surgeon who specializes in knee surgery can determine whether surgery is an appropriate option.
In addition to recommending a specific surgery or set of surgeries, the surgeon will explain the surgery’s potential benefits, expected recovery period, and potential risks and side effects, as well as alternatives to the surgery. Once fully informed, the patient can decide whether or not to have the surgery.
Disclaimer: This article has been taken from https://www.arthritis-health.com/ as it is. Click here to read the original article.
The posterior cruciate ligament (PCL) is the strongest ligament in the knee joint. Ligaments are thick, strong bands of tissue that connect bone to bone. The PCL runs along the back of the knee joint from the bottom of the thighbone (femur) to the top of the lower leg bone (tibia).
The PCL helps keep the knee joint stable, especially the back of the joint. An injury to the PCL could involve straining, spraining, or tearing any part of that ligament. The PCL is the least commonly injured ligament in the knee.
A PCL injury is sometimes referred to as an “overextended knee.”
What Causes a PCL Injury?
The main cause of PCL injury is severe trauma to the knee joint. Often, other ligaments in the knee are affected as well. One cause specific to PCL injury is hyperextension of the knee. This can occur during athletic movements like jumping.
PCL injuries can also result from a blow to the knee while it is flexed, or bent. This includes landing hard during sports or a fall, or from a car accident. Any trauma to the knee, whether minor or severe, can cause a knee ligament injury.
Symptoms of a PCL Injury
Symptoms of a PCL injury can be mild or severe, depending on the extent of the injury. Symptoms might be nonexistent if the ligament is mildly sprained. For a partial tear or complete tear of the ligament, common symptoms include:
tenderness in the knee (specifically the back of the knee)
instability in the knee joint
pain in the knee joint
swelling in the knee
stiffness in the joint
difficulty walking
Diagnosing a PCL Injury
To diagnose a PCL injury, your doctor will perform a variety of tests, including:
moving the knee in various directions
physical examination of the knee
checking for fluid in the knee joint
an MRI of the knee
an X-ray of the knee joint to check for fractures
Preventing a PCL Injury
It’s difficult to prevent ligament injuries because they are often the result of an accident or unforeseen circumstance. However, preventive measures that can be taken to help minimize the risk of a knee ligament injury include:
using proper technique and alignment when doing physical activities, including walking
stretching regularly to maintain good range of motion in the joints
strengthening the muscles of the upper and lower legs to help stabilize the joint
using caution when playing sports in which knee injuries are common like football, skiing, and tennis
Treating PCL Injuries
The treatment for PCL injuries will depend on the severity of the injury and your lifestyle.
For minor injuries, treatment may include:
splinting
applying ice
elevating the knee above the heart
taking a pain reliever
limiting physical activity until pain and swelling are gone
using a brace or crutches to protect the knee
physical therapy or rehabilitation to strengthen and regain range of motion
In more severe cases, treatment may also include:
physical therapy or rehabilitation to strengthen and regain range of motion
surgery to repair a torn ligament
an arthroscope, a small fiber-optic camera that can be inserted into the joint
The major symptom of posterior cruciate ligament PCL injuries is joint instability. Many of the other symptoms, including pain and swelling, will go away with time, but instability may remain. In PCL injuries, this instability is often what leads people to elect surgery. Untreated instability in the joint may lead to arthritis.
Outlook for a PCL Injury
For minor injuries, the ligament may heal without complications. It’s important to note that if the ligament was stretched, it may never regain its prior stability. This means it’s more likely that the knee may be somewhat unstable and could be easily injured again. The joint could become swollen and sore simply from physical activity or minor injury.
For those with major injuries who don’t have surgery, the joint will most likely remain unstable and be easily reinjured. You will be less able to do physical activities and pain could result from even minor activities. You may have to wear a brace to protect the joint during physical activity.
For those who have surgery, the prognosis depends on the success of the surgery and of the associated injuries to the knee. Generally, you will have improved mobility and stability after the joint is repaired. You may need to wear a brace or limit physical activities in the future to help prevent reinjuring the knee.
For knee injuries involving more than just the posterior cruciate ligament PCL, treatment and prognosis may be different because those injuries maybe more severe
Disclaimer: This article has been taken from https://www.healthline.com// as it is. Click here to read the original article.
The posterior cruciate ligament (PCL), is one of four ligaments important to the stability of the knee joint. There many Posterior Cruciate Ligament Treatment. The anterior cruciate ligament (ACL), sits just in front of the PCL. The ACL is much better known, in part because ACL tears are much more commonly diagnosed than injuries to the PCL. Interestingly, it is thought that PCL injuries account for up to 20 percent of knee ligament injuries, however, the PCL is seldom talked about because these injuries are often left undiagnosed.1
The PCL is the ligament that prevents the tibia (shin bone) from sliding too far backward. Along with the ACL which keeps the tibia from sliding too far forward, the PCL helps to maintain the tibia in a position below the femur (thigh bone).
PCL Tears
The most common mechanism of injury of the PCL is the so-called “dashboard injury.”1 This occurs when the knee is bent, and an object forcefully strikes the shin backward. It is called a ‘dashboard injury’ because this can be seen in car collisions when the shin forcefully strikes the dashboard. The other common mechanism of injury is a sports injury when an athlete falls on the front of their knee. In this injury, the knee is hyper flexed (bent all the way back), with the foot held pointing downwards. These types of injuries stress the PCL, and if the force is high enough, a PCL tear can be the result.
PCL injuries are also commonly seen with severe trauma that can cause injury to many knee structures. PCL tears can be associated with other knee ligament injuries, including ACL tears, MCL tears, and LCL tears.2 They can also be found with complex ligament injury patterns such as posterolateral rotatory instability. In addition, PCL injuries may be associated with meniscus tears and cartilage damage. Often these more severe patterns of injury occur with a knee dislocation.
Symptoms of PCL Tears
The most common symptoms of a PCL tear are quite similar to the symptoms of an ACL tear. Knee pain, swelling and decreased motion are common with both injuries.1 Patients may have a sensation that their knee “popped” or gave out. Problems with knee instability in the weeks and months following PCL injury are not as common as instability following an ACL tear. When patients have instability after a PCL injury they usually state that they can’t “trust” their knee, or that it feels as though the knee may give out. If this complaint of instability is a problem after a PCL injury, it may be an indication to proceed with surgery.
The major factor in making the diagnosis of a PCL tear is by knowing how the injury happened. Knowing the story of the injury (for example, the position of the leg and the action taking place) will help in making the diagnosis. Specific maneuvers can test the function of the PCL. The most reliable is the posterior drawer test.2 With the knee bent, your doctor will push the tibia backward; this stresses the PCL. If the PCL is deficient or torn, the tibia will slide too far backward, and indicate an injury to the PCL.
X-rays and MRIs are also helpful in clarifying the diagnosis and detecting any other structures of the knee that may be injured. It is common to find other ligament injuries or cartilage damage when a PCL tear is found.
PCL tears are graded by the severity of the injury, grade I through grade III.2 The grade is determined by the extent of laxity measured during your examination. In general, grading of the injury corresponds to the following:
Grade I: Partial tears of the PCL.
Grade II: Isolated, complete tear to the PCL.
Grade III: Tear of the PCL with other associated ligament injuries.
Treatment of a PCL Tear
Posterior Cruciate Ligament Treatment & tears is controversial, and, unlike the treatment of an ACL tear, there is little agreement about the optimal treatment for all patients.1 Initial treatment of the pain and swelling consists of the use of crutches, ice, and elevation. Once these symptoms have settled, physical therapy is beneficial to improve knee motion and strength. Nonoperative treatment is recommended for most grade I and grade II PCL tears.
Surgical reconstruction of the PCL is controversial, and usually only recommended for grade III PCL tears. Because of the technical difficulty of the surgery, some orthopedic surgeons do not see the benefit of PCL reconstruction. Others, however, believe PCL reconstruction can lead to improved knee stability and lower the likelihood of problems down the road.
Posterior Cruciate Ligament Treatment in surgery reconstruction is difficult in part because of the position of the PCL in the knee. Trying to place a new PCL graft in this position is difficult, and over time these grafts are notorious for stretching out and becoming less functional. Generally, surgical PCL reconstruction is reserved for patients who have injured several major knee ligaments, or for those who cannot do their usual activities because of persistent knee instability.
Disclaimer: This article has been taken from https://www.verywellhealth.com/ as it is. Click here to read the original article.
What Is It?
The posterior cruciate ligament (PCL) and the anterior cruciate ligament (ACL) are two tough bands of fibrous tissue that connect the thighbone (femur) and the large bone of the lower leg (tibia) at the knee joint. Together, the ACL and PCL bridge the inside of the knee joint, forming an “X” pattern that stabilizes the knee against front-to-back and back-to-front forces. In particular, the PCL prevents the lower leg from slipping too far back in relation to the upper leg, especially when the knee is flexed (bent).
Posterior Cruciate Ligament (PCL) Injuries includes a stretch or tear of the ligament. The Posterior Cruciate Ligament (PCL) Injuries most often occurred when the front of the knee hits the dashboard during an automobile accident. During sports activities, the PCL also can tear when an athlete falls forward and lands hard on a bent knee, which is common in football, basketball, soccer and especially rugby.
Disclaimer: This article has been taken from https://www.health.harvard.edu/ as it is. Click here to read the original article.


 Knee Osteoarthritis Video
Knee Osteoarthritis Video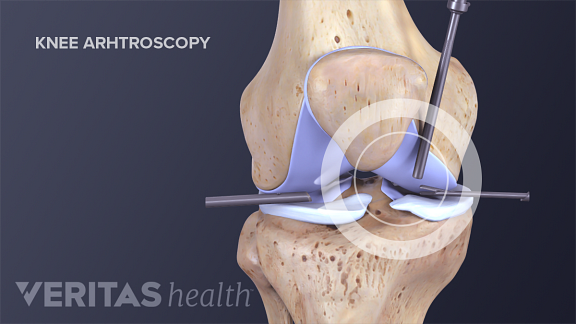

:max_bytes(150000):strip_icc():format(webp)/GettyImages-804436012-de279a2a929643beaa9684b1b2f68d47.jpg)
