A liver transplant, also called a hepatic transplant, can help save your life when your liver no longer works. The treatment involves surgical removal of your entire liver. It’s then replaced with all, or part, of a healthy donor liver. This may come from a living or deceased donor.
Having a healthy liver is essential to longevity because your liver is responsible for filtering blood and removing toxins from your body. Liver transplant is a last-resort measure for chronic (long-term) liver diseases and severe acute (sudden onset) liver diseases.
Liver transplant survival statistics
According to a studyTrusted Source, people who have a liver transplant have an 89% percent chance of living after one year. The five-year survival rate is 75 percentTrusted Source. Sometimes the transplanted liver can fail, or the original disease may return.
It’s important that your doctor monitors your recovery long after the transplant to detect any problems. You’ll likely need regular blood tests. According to Johns Hopkins, you’ll also need to take antirejection medications for the rest of your life.
Why liver transplants are done
According to the American Liver Foundation, around 8,000 liver transplant surgeries are performed in the United States every year.
A doctor may recommend a liver transplant for a person with end-stage liver disease. A person with this condition will die without a transplant. A doctor may also suggest a liver transplant if other treatments for liver disease aren’t enough to keep a person alive.
Liver transplants may be option for chronic liver disease or if liver failure happens very quickly. Cirrhosis is the most common reason why adults need liver transplants. Cirrhosis replaces healthy liver tissue with scarred tissue. Causes of cirrhosis include:
Before granting a liver transplant, a doctor will weigh whether the surgery will be successful and extend a person’s life. A person may not be a likely transplant candidate if they have other chronic conditions that could affect a transplant’s success.
Examples include a person who has cancer that has spread to other body parts or has severe heart problems. As another example, if a person has cirrhosis from alcoholism, their ability to quit drinking is evaluated as part of the transplant planning.
Waiting for a liver transplant
If you become eligible for a liver transplant, you’ll be placed on a national waiting list. As of early 2015, an estimated 14,000 peopleTrusted Source in the United States were awaiting liver transplants.
List placement and waiting for a match
Where you’re placed on the list is in part decided by a Model of End-Stage Liver Disease (MELD) score. This score is based on blood tests, such as:
measuring your level of creatinine, which shows how well your kidneys are working
checking your international normalized ratio, which is a measure of how well your liver is making blood-clotting proteins
Those with the highest scores are sicker, and they are placed higher on the list. Regular blood tests are necessary to update your MELD score and position on the list. There is also a Pediatric End-Stage Liver Disease score for those younger than age 12. Transplant surgery’s success also depends on a good match with a qualifying donor, so your wait time may also vary based on your body size and blood type.
Various factors determine whether a person receives a liver transplant. For instance, if two people with high MELD scores qualify for a liver transplant, the person who has been on the list the longest may receive a transplant sooner. In addition, a person high on the transplant list who has a rare blood type may be less likely to match with a donor.
A person experiencing acute liver failure may be placed near the top of the list because their risk of death could be more imminent compared to someone with a chronic condition.
When a match is found
Waiting for a liver transplant is a long process, but the surgery coordination happens quickly once you have a match. The liver can come from a deceased donor who had a healthy liver. Sometimes a donated liver may be used for two recipients. The right side of the donated organ is more often used in adult recipients, while the smaller left side is more often used for children.
It’s possible that a living donor can donate a portion of their liver as well. However, the living donor must be a good match in terms of blood type and other factors.
Recovering from a liver transplant
Getting the transplant is just a part of the process of getting a new liver. According to the National Institute of Diabetes and Digestive and Kidney Diseases, a three-week hospital stay is common after a transplant. During this time, your doctor will evaluate the success of your operation, as well as determine your needs for home care.
It may take up to one year until you feel healthier. Let your doctor know what your mental and emotional health needs are before you’re discharged.
Possible risks and complications of a liver transplant
The greatest risk of this operation is transplant failure. In such a case, your body rejects the new liver, often for reasons doctors can’t determine. A liver transplant also puts you at a high risk for infection. Other long-term complications can include:
side effects from medications taken to allow your immune system to accept the new liver, including high blood sugar from steroids
Healthy liver tips
After a liver transplant, your doctor may recommend lifestyle changes, including regular exercise and a healthy diet. You can incorporate habits like these at any stage to boost your strength and overall health. Being physically healthy may reduce your chances for transplant rejection.
You can also limit risk factors that contribute to liver disease. Among the most common are:
Disclaimer: This article has been taken from https://www.healthline.com/ as it is. Click here to read the original article.
What Is In Vitro Fertilization?
In Vitro Fertilization (IVF) is a type of assistive reproductive technology (ART). It involves retrieving eggs from a woman’s ovaries and fertilizing them with sperm. This fertilized egg is known as an embryo. The embryo can then be frozen for storage or transferred to a woman’s uterus.
Depending on your situation, IVF can use:
your eggs and your partner’s sperm
your eggs and donor sperm
donor eggs and your partner’s sperm
donor eggs and donor sperm
donated embryos
Your doctor can also implant embryos in a surrogate, or gestational carrier. This is a woman who carries your baby for you.
The success rate of IVF varies. According to the American Pregnancy Association, the live birth rate for women under age 35 undergoing IVF is 41 to 43 percent. This rate falls to 13 to 18 percent for women over the age of 40.
Why Is In Vitro Fertilization Performed?
IVF helps people with infertility who want to have a baby. In Vitro Fertilization (IVF) is expensive and invasive, so couples often try other fertility treatments first. These may include taking fertility drugs or having intrauterine insemination. During that procedure, a doctor transfers sperm directly into a woman’s uterus.
Infertility issues for which IVF may be necessary include:
reduced fertility in women over the age of 40
blocked or damaged fallopian tubes
reduced ovarian function
endometriosis
uterine fibroids
male infertility, such as low sperm count or abnormalities in sperm shape
unexplained infertility
Parents may also choose IVF if they run the risk of passing a genetic disorder on to their offspring. A medical lab can test the embryos for genetic abnormalities. Then, a doctor only implants embryos without genetic defects.
How Do I Prepare for In Vitro Fertilization?
Before beginning IVF, women will first undergo ovarian reserve testing. This involves taking a blood sample and testing it for the level of follicle stimulating hormone (FSH). The results of this test will give your doctor information about the size and quality of your eggs.
Your doctor will also examine your uterus. This may involve doing an ultrasound, which uses high-frequency sound waves to create an image of your uterus. Your doctor may also insert a scope through your vagina and into your uterus. These tests can reveal the health of your uterus and help the doctor determine the best way to implant the embryos.
Men will need to have sperm testing. This involves giving a semen sample, which a lab will analyze for the number, size, and shape of the sperm. If the sperm are weak or damaged, a procedure called intracytoplasmic sperm injection (ICSI) may be necessary. During ICSI, a technician injects sperm directly into the egg. ICSI can be part of the IVF process.
Choosing to have IVF is a very personal decision. There are a number of factors to consider.
What will you do with any unused embryos?
How many embryos do you wish to transfer? The more embryos transferred, the higher the risk of a multiple pregnancy. Most doctors won’t transfer more than two embryos.
How do you feel about the possibility of having twins, triplets, or a higher order multiple pregnancy?
What about the legal and emotional issues associated with using donated eggs, sperm, and embryos or a surrogate?
What are the financial, physical, and emotional stresses associated with IVF?
How Is In Vitro Fertilization Performed?
There are five steps involved in IVF:
stimulation
egg retrieval
insemination
embryo culture
transfer
Stimulation
A woman normally produces one egg during each menstrual cycle. However, IVF requires multiple eggs. Using multiple eggs increases the chances of developing a viable embryo. You’ll receive fertility drugs to increase the number of eggs your body produces. During this time, your doctor will perform regular blood tests and ultrasounds to monitor the production of eggs and to let your doctor know when to retrieve them.
Egg Retrieval
Egg retrieval is known as follicular aspiration. It’s a surgical procedure performed with anesthesia. Your doctor will use an ultrasound wand to guide a needle through your vagina, into your ovary, and into an egg-containing follicle. The needle will suction eggs and fluid out of each follicle.
Insemination
The male partner will now need to give a semen sample. A technician will mix the sperm with the eggs in a petri dish. If that doesn’t produce embryos, your doctor may decide to use ICSI.
Embryo Culture
Your doctor will monitor the fertilized eggs to ensure that they’re dividing and developing. The embryos may undergo testing for genetic conditions at this time.
Transfer
When the embryos are big enough, they can be implanted. This normally occurs three to five days after fertilization. Implantation involves inserting a thin tube called a catheter inserted into your vagina, past your cervix, and into your uterus. Your doctor then releases the embryo into your uterus.
Pregnancy occurs when the embryo implants itself in the uterine wall. This can take 6 to 10 days. A blood test will determine if you’re pregnant.
What Are the Complications Associated with In Vitro Fertilization IVF?
As with any medical procedure, there are risks associated with IVF. Complications include:
multiple pregnancies, which increases the risk of low birth weight and premature birth
miscarriage (pregnancy loss)
ectopic pregnancy (when the eggs implant outside the uterus)
ovarian hyperstimulation syndrome (OHSS), a rare condition involving an excess of fluid in the abdomen and chest
bleeding, infection, or damage to the bowels or bladder (rare)
What Is the Long-Term Outlook?
Deciding whether to undergo in vitro fertilization, and how to try if the first attempt is unsuccessful, is an incredibly complicated decision. The financial, physical, and emotional toll of this process can be difficult. Speak with your doctor extensively to determine what your best options are and if in vitro fertilization is the right path for you and your family. Seek a support group or counselor to help you and your partner through this process.
Disclaimer: This article has been taken from https://www.healthline.com/ as it is. Click here to read the original article.
A brain tumor is a collection, or mass, of abnormal cells in your brain. Your skull, which encloses your brain, is very rigid. Any growth inside such a restricted space can cause problems. Brain tumors can be cancerous (malignant) or noncancerous (benign). When benign or malignant tumors grow, they can cause the pressure inside your skull to increase. This can cause brain damage, and it can be life-threatening.
Brain tumors are categorized as primary or secondary. A primary brain tumor originates in your brain. Many primary brain tumors are benign. A secondary brain tumor, also known as a metastatic brain tumor, occurs when cancer cells spread to your brain from another organ, such as your lung or breast.
Types of brain tumors
Primary brain tumors
Primary brain tumors originate in your brain. They can develop from your:
brain cells
the membranes that surround your brain, which are called meninges
nerve cells
glands
Primary tumors can be benign or cancerous. In adults, the most common types of brain tumors are gliomas and meningiomas.
Gliomas
Gliomas are tumors that develop from glial cells. These cells normally:
support the structure of your central nervous system
provide nutrition to your central nervous system
clean cellular waste
break down dead neurons
Gliomas can develop from different types of glial cells.
The types of tumors that begin in glial cells are:
astrocytic tumors such as astrocytomas, which originate in the cerebrum
oligodendroglial tumors, which are often found in the frontal temporal lobes
glioblastomas, which originate in the supportive brain tissue and are the most aggressive type
Other primary brain tumors
Other primary brain tumors include:
pituitary tumors, which are usually benign
pineal gland tumors, which can be benign or malignant
ependymomas, which are usually benign
craniopharyngiomas, which occur mostly in children and are benign but can have clinical symptoms like changes in vision and premature puberty
primary central nervous system (CNS) lymphomas, which are malignant
primary germ cell tumors of the brain, which can be benign or malignant
meningiomas, which originate in the meninges
schwannomas, which originate in cells that produce the protective cover of your nerves (myelin sheath) called Schwann cells
Most meningiomas and schwannomas occur in people between the ages of 40 and 70. Meningiomas are more common in women than men. Schwannomas occur equally in both men and women. These tumors are usually benign, but they can cause complications because of their size and location. Cancerous meningiomas and schwannomas are rare but can be very aggressive.
Secondary brain tumors
Secondary brain tumors make up the majority of brain cancers. They start in one part of the body and spread, or metastasize, to the brain. The following can metastasize to the brain:
lung cancer
breast cancer
kidney cancer
skin cancer
Secondary brain tumors are always malignant. Benign tumors don’t spread from one part of your body to another.
What are the risk factors for a brain tumor?
Risk factors for brain tumors include:
Family history
Only about 5 to 10 percent of all cancers are genetically inherited, or hereditary. It’s rare for a brain tumor to be genetically inherited. Talk to your doctor if several people in your family have been diagnosed with a brain tumor. Your doctor can recommend a genetic counselor for you.
Age
Risk for most types of brain tumors increases with age.
Race
Brain tumors in general are more common among Caucasians. However, African-American people are more likely to get meningiomas.
People who have been exposed to ionizing radiation have an increased risk of brain tumors. You can be exposed to ionizing radiation through high-radiation cancer therapies. You can also be exposed to radiation from nuclear fallout. The nuclear power plant incidents in Fukushima and Chernobyl are examples of how people can be exposed to ionizing radiation.
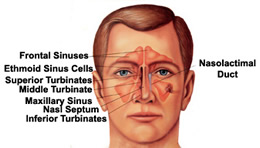
Sinusitis is one of the most common chronic (ongoing) conditions in the United States effecting fifty million Americans, 20% of the nation’s population.
Sinusitis is often a chronic (ongoing) disease that includes the symptoms of nasal obstruction (difficulty breathing through the nose), nasal drainage, decreased sense of smell, facial pressure, and frequent sinus infections. Allergies and related respiratory problems such as asthma can also be associated with chronic sinusitis.
It can sometimes be difficult for patients to decipher if they are suffering from allergies, an upper respiratory tract infection, or a sinus condition. Symptoms and signs for each condition differ, and each diagnosis requires a unique treatment regimen. The Oregon Sinus Center team can help make an informed choice as to the best management strategy for a patient with any of these conditions.
After getting the correct diagnosis, a number of medical treatments can be started. These medications may include anti-inflammatory nasal sprays, decongestants, oral inflammatory inhibitors, and systemic steroid medications. It is important that the physician and patient recognize that medications are often required on a long-term basis.
In some cases, surgery is required using a telescope (endoscope) which is placed through the nostril. This type of surgery is often referred to as Endoscopic Sinus Surgery, which is minimally invasive and does not require any external incisions. It is our goal that after surgery, patients will not require any further surgery on the nose and sinuses.
In some cases, however, sinusitis can return. Our surgeons have a particular interest in patients whose sinusitis has failed traditional surgery and require advanced techniques to control the underlying inflammation. The Oregon Sinus Center actively conducts ongoing research into better treatments for sinusitis.
Nasal & Sinus Polyps
Nasal polyps are associated with sinusitis and occur when the lining of the sinuses swell. Polyps may block the nasal airway, creating difficulty in breathing. Polyps may also block the natural drainage of the sinus cavities leading to infections. Polyps are generally thought to occur as a result of an ongoing inflammatory process within the nose and sinuses.
After getting the correct diagnosis, our team of can help patients decide on the most appropriate treatment plan. Most commonly, medications are tried as first line therapy. Different combinations can be tailored for individual patients. In some cases, a patient’s disease cannot be fully controlled with medication and surgery may be recommended. This surgery is done with telescopes (endoscopes) through the nose in a minimally invasive fashion.
Following this type of surgery, it is very important to maintain medical treatment. Additionally, the nose and sinus cavities must be watched carefully to prevent the return of the polyps. It is our goal that after surgery, patients will not require any further surgery on the nose and sinuses to remove polyps.
In some cases, however, polyps may return. Our surgeons have a particular interest in patients who have experienced the return of polyps following previous nasal and sinus surgeries. We are experts in the more advanced techniques that may be required to control polyp formation. The Oregon Sinus Center actively conducts ongoing research into better treatments for sinus polyps.
Smell and Taste Disorders
Disorders of smell and taste can have a large impact on quality of life. Currently about 2 million adults in the United States are evaluated for smell and taste disorders every year, but it is believed many more cases go unreported. It is estimated that up to 80% of taste is a result of olfactory (or smell) input. As a result, loss of smell is frequently interpreted as a loss of taste.
Problems with smell and taste can be due to a variety of causes. Examples of these include chronic rhinosinusitis, polyps, allergic rhinitis, upper respiratory infection, trauma, tumors or other neurological disorders.
Evaluations of these disorders include a thorough history and physical exam with an endoscope, objective smell testing, and may also include imaging. Treatment of these problems depends on the problem and the severity of the loss. Our team works with each patient to best understand the cause of their smell and taste problems. From there, a therapeutic plan can be initiated.
Disclaimer : This article has been sourced from https://www.ohsu.edu/ as it is. Click here to read original article.
What is a kidney transplant?
A kidney transplant is a surgical procedure that’s done to treat kidney failure. The kidneys filter waste from the blood and remove it from the body through your urine. They also help maintain your body’s fluid and electrolyte balance. If your kidneys stop working, waste builds up in your body and can make you very sick.
People whose kidneys have failed usually undergo a treatment called dialysis. This treatment mechanically filters waste that builds up in the bloodstream when the kidneys stop working.
Some people whose kidneys have failed may qualify for a kidney transplant. In this procedure, one or both kidneys are replaced with donor kidneys from a live or deceased person.
There are pros and cons to both dialysis and kidney transplants.
Undergoing dialysis takes time and is labor-intensive. Dialysis often requires making frequent trips to a dialysis center to receive treatment. At the dialysis center, your blood is cleansed using a dialysis machine.
If you’re a candidate to have dialysis in your home, you’ll need to purchase dialysis supplies and learn how to use them.
A kidney transplant can free you from a long-term dependence on a dialysis machine and the strict schedule that goes with it. This can allow you to live a more active life. However, kidney transplants aren’t suitable for everyone. This includes people with active infections and those who are severely overweight.
During a kidney transplant, your surgeon will take a donated kidney and place it in your body. Even though you’re born with two kidneys, you can lead a healthy life with only one functioning kidney. After the transplant, you’ll have to take immune-suppressing medications to keep your immune system from attacking the new organ.
Who might need a kidney transplant?
A kidney transplant may be an option if your kidneys have stopped working entirely. This condition is called end-stage renal disease (ESRD) or end-stage kidney disease (ESKD). If you reach this point, your doctor is likely to recommend dialysis.
In addition to putting you on dialysis, your doctor will tell you if they think you’re a good candidate for a kidney transplant.
You’ll need to be healthy enough to have major surgery and tolerate a strict, lifelong medication regimen after surgery to be a good candidate for a transplant. You must also be willing and able to follow all instructions from your doctor and take your medications regularly.
If you have a serious underlying medical condition, a kidney transplant might be dangerous or unlikely to be successful. These serious conditions include:
Your doctor may also recommend that you don’t have a transplant if you:
smoke
drink alcohol in excess
use illicit drugs
If your doctor thinks you’re a good candidate for a transplant and you’re interested in the procedure, you’ll need to be evaluated at a transplant center.
This evaluation usually involves several visits to assess your physical, psychological, and familial condition. The center’s doctors will run tests on your blood and urine. They’ll also give you a complete physical exam to ensure you’re healthy enough for surgery.
A psychologist and a social worker will also meet with you to make sure you’re able to understand and follow a complicated treatment regimen. The social worker will make sure you can afford the procedure and that you have adequate support after you’re released from the hospital.
If you’re approved for a transplant, either a family member can donate a kidney or you’ll be placed on a waiting list with the Organ Procurement and Transplantation Network (OPTN). The typical wait for a deceased donor organ is over five years.
Who donates the kidney?
Kidney donors may be either living or deceased.
Living donors
Because the body can function perfectly well with just one healthy kidney, a family member with two healthy kidneys may choose to donate one of them to you.
If your family member’s blood and tissues match your blood and tissues, you can schedule a planned donation.
Receiving a kidney from a family member is a good option. It reduces the risk that your body will reject the kidney, and it enables you to bypass the multiyear waiting list for a deceased donor.
Deceased donors
Deceased donors are also called cadaver donors. These are people who have died, usually as the result of an accident rather than a disease. Either the donor or their family has chosen to donate their organs and tissues.
Your body is more likely to reject a kidney from an unrelated donor. However, a cadaver organ is a good alternative if you don’t have a family member or friend who’s willing or able to donate a kidney.
The matching process
During your evaluation for a transplant, you’ll have blood tests to determine your blood type (A, B, AB, or O) and your human leukocyte antigen (HLA). HLA is a group of antigens located on the surface of your white blood cells. Antigens are responsible for your body’s immune response.
If your HLA type matches the donor’s HLA type, it’s more likely that your body won’t reject the kidney. Each person has six antigens, three from each biological parent. The more antigens you have that match those of the donor, the greater the chance of a successful transplant.
Once a potential donor is identified, you’ll need another test to make sure that your antibodies won’t attack the donor’s organ. This is done by mixing a small amount of your blood with the donor’s blood.
The transplant can’t be done if your blood forms antibodies in response to the donor’s blood.
If your blood shows no antibody reaction, you have what’s called a “negative crossmatch.” This means that the transplant can proceed.
What is kidney transplant procedure?
Your doctor can schedule the transplant in advance if you’re receiving a kidney from a living donor.
However, if you’re waiting for a deceased donor who’s a close match for your tissue type, you’ll have to be available to rush to the hospital at a moment’s notice when a donor is identified. Many transplant hospitals give their people pagers or cell phones so that they can be reached quickly.
Once you arrive at the transplant center, you’ll need to give a sample of your blood for the antibody test. You’ll be cleared for surgery if the result is a negative crossmatch.
A kidney transplant is done under general anesthesia. This involves giving you a medication that puts you to sleep during the surgery. The anesthetic will be injected into your body through an intravenous (IV) line in your hand or arm.
Once you’re asleep, your doctor makes an incision in your abdomen and places the donor kidney inside. They then connect the arteries and veins from the kidney to your arteries and veins. This will cause blood to start flowing through the new kidney.
Your doctor will also attach the new kidney’s ureter to your bladder so that you’re able to urinate normally. The ureter is the tube that connects your kidney to your bladder.
Your doctor will leave your original kidneys in your body unless they’re causing problems, such as high blood pressure or infection.
Kidney Transplant Procedure Aftercare
You’ll wake up in a recovery room. Hospital staff will monitor your vital signs until they’re sure you’re awake and stable. Then, they’ll transfer you to a hospital room.
Even if you feel great after your transplant (many people do), you’ll likely need to stay in the hospital for up to a week after surgery.
Your new kidney may start to clear waste from the body immediately, or it may take up to a few weeks before it starts functioning. Kidneys donated by family members usually start working more quickly than those from unrelated or deceased donors.
You can expect a good deal of pain and soreness near the incision site while you’re first healing. While you’re in the hospital, your doctors will monitor you for complications. They’ll also put you on a strict schedule of immunosuppressant drugs to stop your body from rejecting the new kidney. You’ll need to take these drugs every day to prevent your body from rejecting the donor kidney.
Before you leave the hospital, your transplant team will give you specific instructions on how and when to take your medications. Make sure that you understand these instructions, and ask as many questions as needed. Your doctors will also create a checkup schedule for you to follow after surgery.
Once you’re discharged, you’ll need to keep regular appointments with your kidney transplant procedure team so that they can evaluate how well your new kidney is functioning.
You’ll need to take your immunosuppressant drugs as directed. Your doctor will also prescribe additional drugs to reduce the risk of infection. Finally, you’ll need to monitor yourself for warning signs that your body has rejected the kidney. These include pain, swelling, and flu-like symptoms.
You’ll need to follow up regularly with your doctor for the first one to two months after surgery. Your recovery may take about six months.
If you want to know what is kidney transplant, then when your kidneys fail, treatment is needed to replace the work your own kidneys can no longer do. There are two types of treatment for kidney failure — dialysis or transplant. Many people feel that a kidney transplant offers more freedom and a better quality of life than dialysis. In making a decision about whether this is the best treatment for you, you may find it helpful to talk to people who already have a kidney transplant. You also need to speak to your doctor, nurse and family members.
When you get a kidney transplant, a healthy kidney is placed inside your body to do the work your own kidneys can no longer do.
On the plus side, there are fewer limits on what you can eat and drink, but you should follow a heart-healthy diet. Your health and energy should improve. In fact, a successful kidney transplant may allow you to live the kind of life you were living before you got kidney disease. Studies show that people with kidney transplants live longer than those who remain on dialysis.
On the minus side, there are the risks of surgery. You will also need to take anti-rejection medicines for as long as your new kidney is working, which can have side effects. You will have a higher risk for infections and certain types of cancer.
Although most transplants are successful and last for many years, how long they last can vary from one person to the next. Many people will need more than one kidney transplant during a lifetime.
What is a “preemptive” or “early” transplant?
Getting a transplant before you need to start dialysis is called a preemptive transplant. It allows you to avoid dialysis altogether. Getting a transplant not long after kidneys fail (but with some time on dialysis) is referred to as an early transplant. Both have benefits. Some research shows that a pre-emptive or early transplant, with little or no time spent on dialysis, can lead to better long-term health. It may also allow you to keep working, save time and money, and have a better quality of life.
Who can get a kidney transplant?
Kidney patients of all ages—from children to seniors—can get a transplant.
You must be healthy enough to have the operation. You must also be free from cancer and infection. Every person being considered for transplant will get a full medical and psychosocial evaluation to make sure they are a good candidate for transplant. The evaluation helps find any problems, so they can be corrected before transplant. For most people, getting a transplant can be a good treatment choice.
What if I’m older or have other health problems?
In many cases, people who are older or have other health conditions like diabetes can still have successful kidney transplants. Careful evaluation is needed to understand and deal with any special risks. You may be asked to do some things that can lessen certain risks and improve the chances of a successful transplant. For example, you may be asked to lose weight or quit smoking.
If you have diabetes, you may also be able to have a pancreas transplant. Ask your healthcare professional about getting a pancreas transplant along with a kidney transplant.
How will I pay for a transplant?
Medicare covers about 80% of the costs associated with an evaluation, transplant operation, follow-up care, and anti-rejection medicines. Private insurers and state programs may cover some costs as well. However, your post-transplant expenses may only be covered for a limited number of years. It’s important to discuss coverage with your social worker, who can answer your questions or direct you to others who can help. Click here to learn more about insurance and transplant.
Getting a Transplant
How do I start the process of getting a kidney transplant?
Ask your healthcare provider to refer you to a transplant center for an evaluation, or contact a transplant center in your area. Any kidney patient can ask for an evaluation.
How does the evaluation process work?
Medical professionals will give you a complete physical exam, review your health records, and order a series of tests and X-rays to learn about your overall health. Everything that can affect how well you can handle treatment will be checked. The evaluation process for a transplant is very thorough. Your healthcare team will need to know a lot about you to help them—and you—decide if a transplant is right for you. One thing you can do to speed the process is to get all the testing done as quickly as possible and stay in close contact with the transplant team. If you’re told you might not be right for a transplant, don’t be afraid to ask why—or if you might be eligible at some future time or at another center. Remember, being active in your own care is one of the best ways to stay healthy.
If someone you know would like to donate a kidney to you, that person will also need to go through a screening to find out if he or she is a match and healthy enough to donate.
If it’s your child who has kidney disease, you’ll want to give serious thought to getting a transplant evaluation for him or her. Because transplantation allows children and young adults to develop in as normal a way as possible in their formative years, it can be the best treatment for them.
If the evaluation process shows that a transplant is right for you or your child, the next step is getting a suitable kidney. (See “Finding a Kidney” below.)
What does the operation involve?
You may be surprised to learn that your own kidneys generally aren’t taken out when you get a transplant. The surgeon leaves them where they are unless there is a medical reason to remove them. The donated kidney is placed into your lower abdomen (belly), where it’s easiest to connect it to your important blood vessels and bladder. Putting the new kidney in your abdomen also makes it easier to take care of any problems that might come up.
The operation takes about four hours. You’ll be sore at first, but you should be out of bed in a day or so, and home within a week. If the kidney came from a living donor, it should start to work very quickly. A kidney from a deceased donor can take longer to start working—two to four weeks or more. If that happens, you may need dialysis until the kidney begins to work.
After surgery, you’ll be taught about the medicines you’ll have to take and their side effects. You’ll also learn about diet. If you’ve been on dialysis, you’ll find that there are fewer restrictions on what you can eat and drink, which is one of the benefits of a transplant.
What are anti-rejection medicines?
Normally, your body fights off anything that isn’t part of itself, like germs and viruses. That system of protection is called your immune system. To stop your body from attacking or rejecting the donated kidney, you will have to take medicines to keep your immune system less active (called anti-rejection medicines or immunosuppressant medicines). You’ll need to take them as long as your new kidney is working. Without them, your immune system would see the donated kidney as “foreign,” and would attack and destroy it.
Anti-rejection medicines can have some side effects. It is important to talk to your healthcare provider about them, so that you know what to expect. Fortunately, for most people, side effects are usually manageable. Changing the dose or type of medicine can often ease some of the side effects.
Besides the immunosuppressive medicines, you will take other medicines as well. You will take medicines to protect you from infection, too. Most people find taking medicines a small trade for the freedom and quality of life that a successful transplant can provide.
After Your Transplant
What happens after I go home?
Once you are home from the hospital, the most important work begins—the follow-up. For your transplant to be successful, you will have regular checkups, especially during the first year. At first, you may need blood tests several times a week. After that, you’ll need fewer checkups, but enough to make sure that your kidney is working well and that you have the right amount of anti-rejection medication in your body.
What if my body tries to reject the new kidney?
One thing that you and your healthcare team will watch for is acute rejection, which means that your body is suddenly trying to reject the transplanted kidney. A rejection episode may not have any clear signs or symptoms. That is why it is so important to have regular blood tests to check how well your kidney is working. Things you might notice that can let you know you are having rejection are fevers, decreased urine output, swelling, weight gain, and pain over your kidney.
The chances of having a rejection episode are highest right after your surgery. The longer you have the kidney, the lower the chance that this will happen. Unfortunately, sometimes a rejection episode happens even if you’re doing everything you’re supposed to do. Sometimes the body just doesn’t accept the transplanted kidney. But even if a rejection episode happens, there are many ways to treat it so you do not lose your transplant. Letting your transplant team know right away that you think you have symptoms of rejection is very important.
How often do rejection episodes happen?
Rejections happen much less often nowadays. That’s because there have been many improvements in immunosuppressive medicines. However, the risk of rejection is different for every person. For most people, rejection can be stopped with special anti-rejection medicines. It’s very important to have regular checkups to see how well your kidney is working, and make sure you are not having rejection.
When can I return to work?
How soon you can return to work depends on your recovery, the kind of work you do, and your other medical conditions. Many people can return to work eight weeks or more after their transplant. Your transplant team will help you decide when you can go back to work.
Will my sex life be affected?
People who have not had satisfactory sexual relations due to kidney disease may notice an improvement as they begin to feel better. In addition, fertility (the ability to conceive children) tends to increase. Men who have had a kidney transplant have fathered healthy children, and women with kidney transplants have had successful pregnancies. It’s best to talk to your healthcare practitioner when considering having a child.
Women should avoid becoming pregnant too soon after a transplant. Most centers want women to wait a year or more. All pregnancies must be planned. Certain medications that can harm a developing baby must be stopped six weeks before trying to get pregnant. Birth control counseling may be helpful. It’s important to protect yourself against sexually transmitted diseases (STDs). Be sure to use protection during sexual activity.
Will I need to follow a special diet?
In general, transplant recipients should eat a heart-healthy diet (low fat, low salt) and drink plenty of fluids. If you have diabetes or other health problems, you may still have some dietary restrictions. A dietitian can help you plan meals that are right for you.
Finding a Kidney
Where do donated kidneys come from?
A donated kidney may come from someone who died and donated a healthy kidney. A person who has died and donated a kidney is called a deceased donor.
Donated kidneys also can come from a living donor. This person may be a blood relative (like a brother or sister) or non-blood relative (like a husband or wife). They can also come from a friend or even a stranger.
When a kidney is donated by a living person, the operations are done on the same day and can be scheduled at a convenient time for both the patient and the donor. A healthy person who donates a kidney can live a normal life with the one kidney that is left. But the operation is major surgery for the donor, as well as the recipient. As in any operation, there are some risks that you will need to consider.
Is it better to get a kidney from a living donor?
Kidneys from living or deceased donors both work well, but getting a kidney from a living donor can work faster and be better. A kidney from a living donor may last longer than one from a deceased donor.
To get a deceased donor kidney, you will be placed on a waiting list once you have been cleared for a transplant. It can take many years for a good donor kidney to be offered to you. From the time you go on the list until a kidney is found, you may have to be on some form of dialysis. While you’re waiting, you’ll need regular blood tests to make sure you are ready when a kidney is found. If you’re on dialysis, your center will make the arrangements for these tests. Your transplant center should know how to reach you at all times. Once a kidney become available, the surgery must be done as soon as possible.
Are there disadvantages to living donation?
A disadvantage of living donation is that a healthy person must undergo surgery to remove a healthy kidney. The donor will need some recovery time before returning to work and other activities. However, recent advances in surgery (often called minimally invasive or laparoroscopic surgery) allow for very small incisions. This means shorter hospital stays and recovery time, less pain, and a quicker return to usual activities. Living donors often experience positive feelings about their courageous gift.
What are the financial costs to the living donor?
The surgery and evaluation is covered by Medicare or the recipient’s insurance. The living donor will not pay for anything related to the surgery. However, neither Medicare nor insurance covers time off from work, travel expenses, lodging, or other incidentals. The National Living Donor Assistance Program (www.livingdonorassistance.org) or other programs may help cover travel and lodging costs.
Donors may be eligible for sick leave, state disability, and benefits under the federal Family Medical Leave Act. In addition, federal employees, some state employees, and certain other workers may be eligible for 30 days paid leave.
Disclaimer : This article has been sourced from https://www.kidney.org/ as it is. Click here to read original article.